
Today is April 16th, 2024, and the US taxes were due yesterday. Have you paid the government?
This time reminds us of the concept “Render unto Caesar“, and the fact that it lies at the foundation of the separation of church and state. Uttered by Jesus in the synoptic gospels the full quote reads, “Render unto Caesar the things that are Caesar’s, and unto God the things that are God’s”. While the words “separation of church and state” do not appear in the U.S. Constitution, the concept is enshrined in the very first freedom guaranteed by the First Amendment: “Congress shall make no law respecting an establishment of religion.”
These statements are foundational for the US culture, and we accept them implicitly. National experience with COVID-19 management has shown the wisdom of applying similar limitations to government management of individual healthcare. It is one thing to collect taxes, and manage resources, it is another to dictate medical approaches. For example, the governments actively pushed vaccination at the expense of established therapeutics. For example, steroids saved more lives in cases of severe, but were not recommended by the NSAID, CDC or the FDA. Below, we summarize some facts, about the COVID experience, and especially reporting. To put it simply not only did governments shut down debate and mandate specific approaches over others, after the fact, they are obviously hiding the damaging reports.
Vaccine development
In the US COVID-19 vaccine was developed in record time under project Warp Speed! And that was the problem. As the graph below shows vaccine development time varies greatly but is typically quite extensive. Notably absent from this list is HIV, which has no vaccine despite being the focus of NSAID’s director Dr. Fauci’s extensive scientific career.
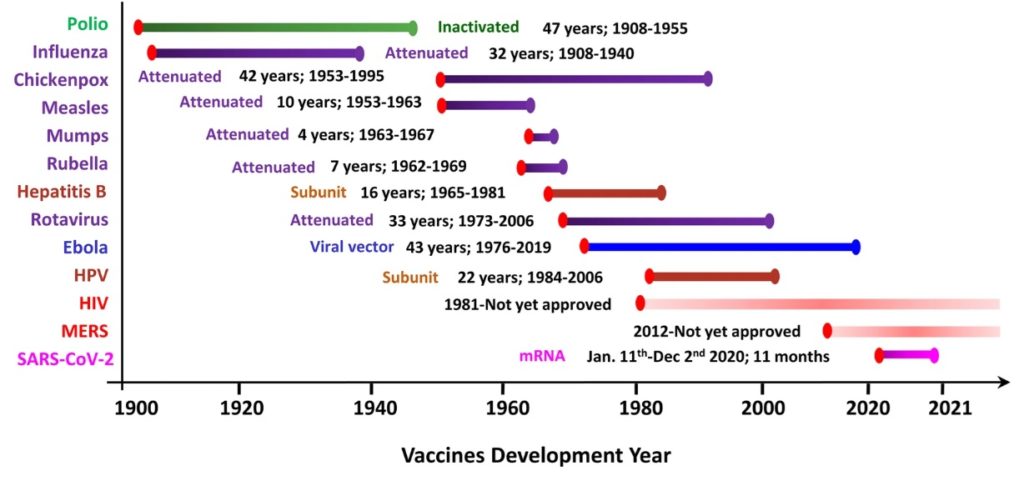
Clearly, testing of COVID-19 vaccine was not completed to the usual standards. Many questions were either not fully explored, or worse the results were hidden. This includes distribution of vaccine in the body, persistence of mRNA in the body, impact on pregnancy, etc.
COVID-19 VAERS data
In fact, the Vaccine Adverse Event Reporting System (VAERS), has long been inaccessible. Some creative researchers found interesting information revealed in VAERS from Australia, however, the US repository has been inaccessible until recently. It is now available, and the raw data can be downloaded here: VAERS – Download Data File (hhs.gov). For your convenience include a screenshot of the data below and our own analysis.
As the screenshot shows, the VAERS system does not actually track information about the nature of the adverse event and its severity. In clinical trials, it is required to record side effects and their severity. Regarding COVID we may inquire, for example, how many vaccine adverse events are related to myocarditis? How severe are they? How frequently do they occur in healthy young men?
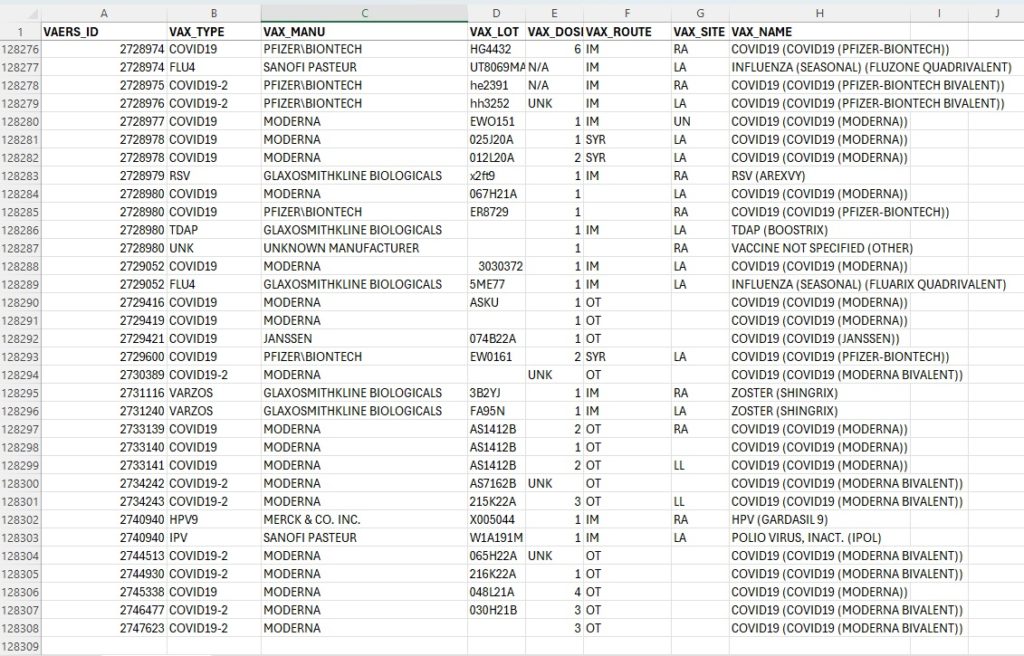
There are over 128,000 VAERS entries and they tell us almost nothing, because the most pertinent information about the nature and severity of adverse events is apparently to collected, or at least not shared.
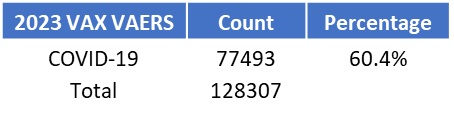
The following presents a short analysis of the few things that can be gleamed from the VAERS data. First, COVID-19 has a lot of associated adverse events, outnumbering all of the other vaccines combined, accounting for over 60% all reports!
If we analyze the adverse events by the number of administered doses, we find that booster (3rd shot and beyond) was associated with higher risks, as is expected from immune sensitization, where repeated injections of mRNA encoding the spike protein led to immune system attacking the body, which is the main form of pathology of COVID. This is why steroids are some helpful for saving lives. The main risks are from over-active immune response, which targets ACE2 receptors in vasculature, the heart and some other organs. Previous experience attempts to make vaccines for SARS-CoV-1 and MERS viruses, closely related to COVID (SARS-CoV-2) has revealed this immune reaction challenge.
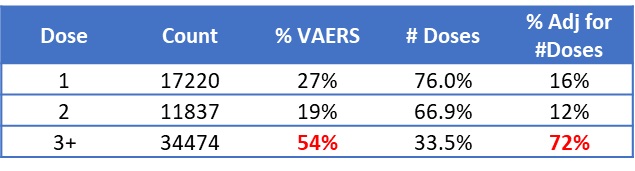
If we adjust for the number of people who have received 3 or more doses (from US Coronavirus vaccine tracker, with state-by-state data) the fraction of adverse events for individuals increases to 72%. Clearly, there are growing risks with additional booster shots.
The impact of additional boosters could not be measured prior to the mass distribution due to the speed of the rollout of the COVID vaccine, nor was this information tracked. In fact, the COVID-19 vaccine was the largest clinical trial in human history, involving over 70% of the global population. It is appropriate to call it a trial, because the full diligence was not done, especially for an entirely new modality of vaccine (mRNA), with unique risk factors.
The government response to the pandemic was first to ignore risks (no human-to-human transmission), mishandle the diagnostic tests, push blanket questionable practices (masks, distancing and lockdowns and vaccinating children as young as 6 months) is now actively hiding the vaccine impact.
Excess deaths post-COVID
There are reports that excess mortality post-COVID in Westen countries that saw mass vaccination has been running 17-20% higher than normal from scientific articles (Assessing the Impact of the Covid-19 Pandemic on US Mortality: A County-Level Analysis – PMC (nih.gov)) and privately including Dr. John Campbell who has devoted many episodes on his popular YouTube channel discussing the dramatic increase in excess deaths. The following table reproduces data from Dr. Campbell’s talks, and the official OEDC data repository with Excess deaths by week, 2020-2023, and CDC data for COVID death total.
The summary below shows that for 2022 and 2023 excess deaths in US and UK dwarfed those of civilians from major military conflicts.

There are many questions about the nature of these excess deaths, however, similar to VAERS data, the critical details of the causes of excess deaths are not recorded. If they were can could track the root causes by analysis of massive national healthcare data.
In summary, the lack of accounting for the handling of the pandemic may have something to do with the vaccine’s adverse impact on health, education, and economics (in the US, the Fed created some $8T from thing air enabling the government paid people to stay home).
Impact of COVID lockdowns on education
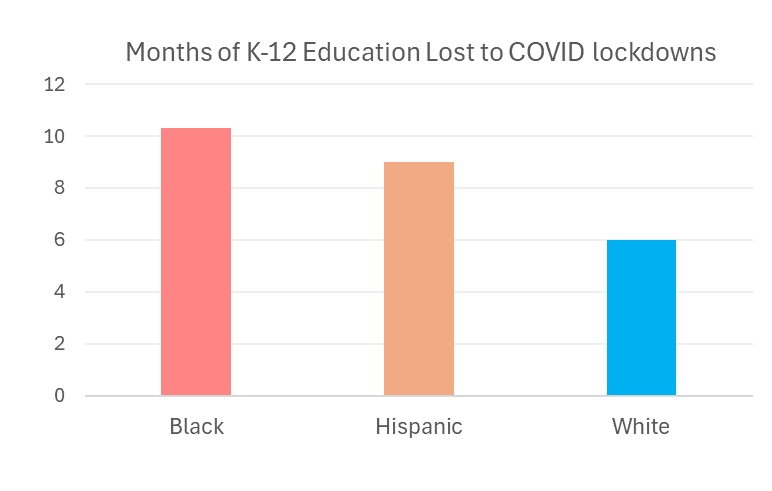
The following is reproduced from Average months of learning lost due to COVID-19 by ethnicity | Statista. As a result of the COVID-19 outbreak, many schools switched to distance learning. Consequently, it is estimated that by June 2023, Black K-12 students lost 10.3 months of learning. Any lost learning due to COVID is regrettable, but this graph shows disparate outcomes by race. Perhaps it is not surprising that the government does not track these statistics, although it both administers the schools and has insisted on lockdowns and mass vaccination. Discussions about detrimental impact of lockdowns of children and their low risks from COVID were stymied during the pandemic, and these sad, shameful results are still not discussed. This impact on the young generation is profound and shows that the government is poorly equipped to make universal decision regarding healthcare.
The better alternative is informed parents make choices for themselves, and their children based on individual needs and risks. Parents are both better informed, and better stewards of their children’s future.
Lockdown alternatives
The national healthcare system in Sweden did not undergo lockdown and experienced lower mortality rate than the US. It also has a national system for tracking healthcare data, which enables it to track very sensitive information, such Long-Term Follow-Up of Transsexual Persons Undergoing Sex Reassignment Surgery: Cohort Study in Sweden | PLOS ONE.
While the Swedish model of government control has its limitations, it appears downright superior to a mixed public-private model in the US that seems to achieve the worst from both worlds. While US citizens are compelled to take vaccines for employment or travel and are subjected to extended lockdowns, we are not able to benefit from a centralized data repository.
Independent massive healthcare data tracking
There are additional opportunities to use massive healthcare data, for example tracking the 20-fold increase of autism prevalence. The government is not leading where it should, in areas of obvious increase of risks, and leading where it should not. Or course, it is difficult for the government to limit its role. They are essential for legal and financial systems but need to leave medicine to professionals and parents. There are exceptional times when the government needs to make broad healthcare decisions, but they should be limited and informed by independent data provided by empowered patients.
If the COVID experience has taught us anything, it is that we should not expect government to play doctor. Similar to how good fences make good neighbors, separation of church and state will make for a better relationship between the citizens and its government.