

Data management and monetization for hospitals
Here we describe how hospitals can monetize their data, while staying in compliance with HIPAA and more recent laws, like Washington state’s My Health, My Data Act. There are two elements necessary: making data transferable and obtaining the patient’s permission. The Sanus platform reimburses patients for data sharing and empowers them to access personalized medicine, making securing such permission very easy. The remaining challenge is primarily a technical one of making data transferable, which means removing all of the specific sources of bias and making the data useful and useable by any medical practitioner, including one with access to different equipment, reagents, personnel, geography, etc.

Data normalization
We present normalization through a simple example of Prostate Specific Antigen (PSA). Consider this situation, as might be described by a doctor: a 65 year old man presents with PSA measured at 4.5ng/mL . . . , but is this actionable ,
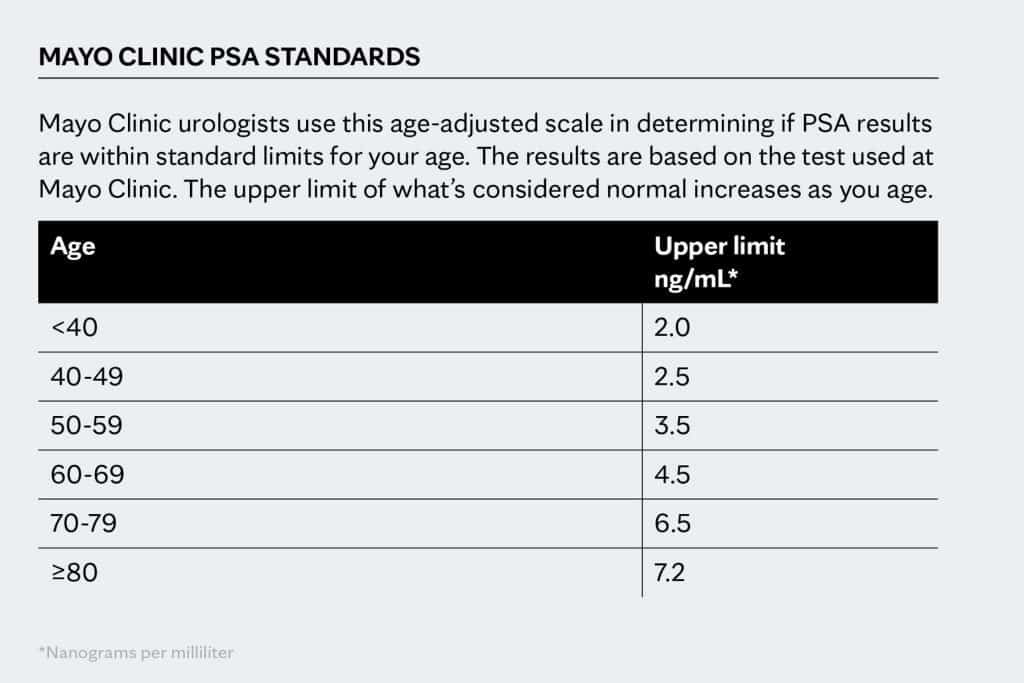
This level of PSA may appear normal on the population level for a man of that age. However, if his baseline measurements over the last two years have been 3ng/mL it is clearly better to represent the measurement in relative terms, namely that the PSA is at 150% of baseline level for the individual.
•Normalization: 4.5ng/mL PSA => 150% PSA
Thus, the measurement reveals elevation of the PSA biomarker by 50% from the baseline level for the individual that appears “normal” at the population level.
In summary, normalization is supposed to take care of patient individuality, as well as different instruments and reagents.
Data optimization
Data optimization is synonymous with data organization and general streamlining of data storage and retrieval. That includes database architecture and meta-data to facilitate medical queries.

Data harmonization
Data harmonization is synonymous with standardization. One example of harmonization in electronic communications is API that helps applications to exchange data. For medical data harmonization requirements are extensive, because there are many factors to account for even after normalization, including the differences in analytes (PSA vs free-PSA, pro-PSA, etc.), sample preparation and data management protocols.
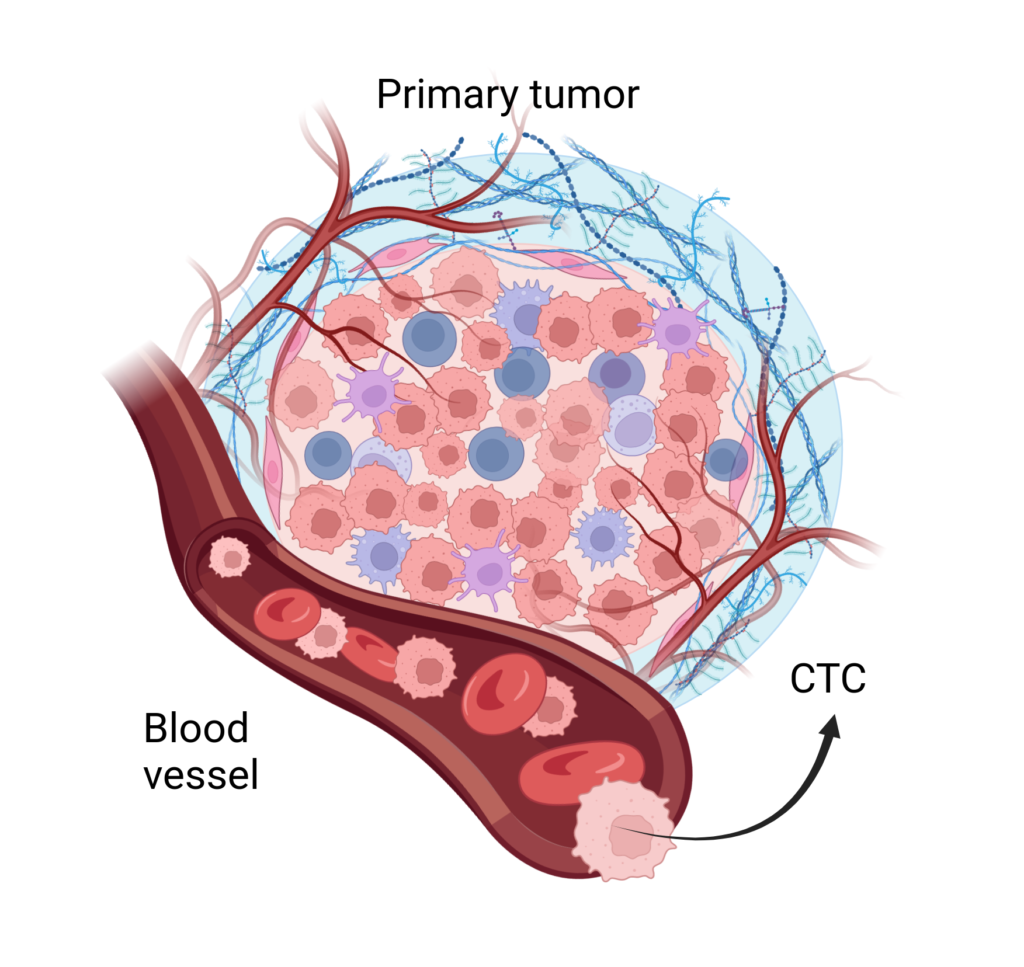
For example, liquid biopsy evidence of cancer can come from a minute amount of DNA from dead cancer cells in the blood, or a few actual cancer cells. There are very different technologies for isolating DNA or Circulating Tumor Cells (CTCs). Regarding the CTCs, identifying a few among billions of native blood cells, relies on different biomarkers, which affect the analysis or even sample preparation.
Data transferability
Data transferability is the ultimate requirement for data sharing. Data is properly formatted, annotated and organized to be transferable. Transferability technically requires the steps described previously: normalization, optimization, and harmonization. The last requirement is consent of the patient, which is achieved by compensating patients for data sharing. Thus, data transferability can lead to data monetization.
Data monetization
Monetization of medical data involves data rental, because it is impossible and improper to separate data from the patient. Therefore, monetization of data requires buy-in from the patient. On the technical side, we describe the steps of preparing the data for transferability.
Sanus provides both the technical tools to help hospitals prepare their data, as well as structures to engage the patient to participate in data sharing.